Paediatric flatfoot is a topic that has sparked much debate over the years, revolving around the decision of when to treat. In this article we will look at the approach taken at Applied Biomechanics, and the evidence that this approach is based on.
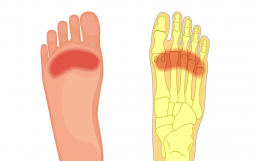
First let’s start by taking a look at what is normal foot development for the paediatric foot. Most kids are born with a flexible flat foot, with a heel (calcaneus) that is in a pronated position (calcaneus is everted, also known as valgus) when in a resting standing position (known as resting calcaneal stance position RCSP). As a child develops the RCSP will correct about a degree a year up until age 7 (Valmassy Formula), with normal being a RSCP of vertical1. This will also correlate with the arch development, which should develop between age 7-102-3
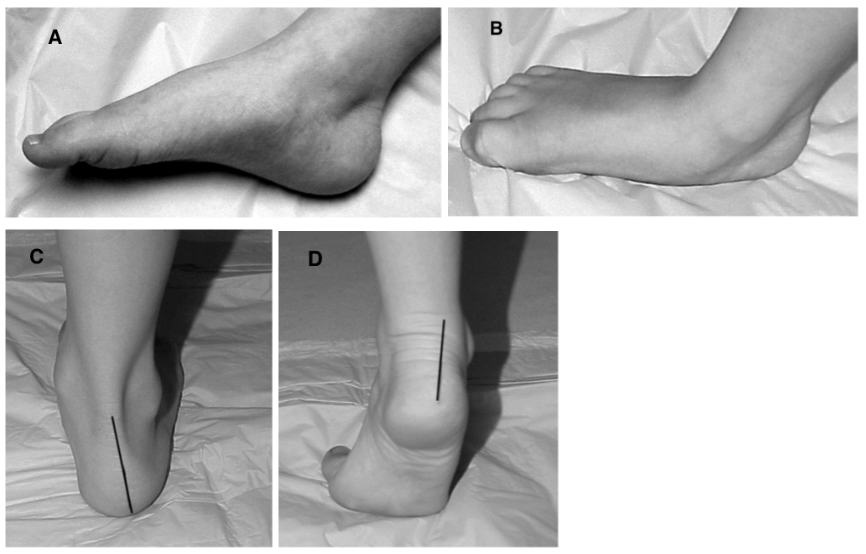
Paediatric feet can be divided into two main categories. Flexible flatfoot, and the rigid flatfoot. The flexible flatfoot is characterized by the reappearance of an arch when the child is sitting on a bench with feet non-weight bearing (Fig 1A,B). An additional test would be to have the child do a heel rise, the arch will reconstitute and the heel will invert in a flexible flatfoot (Fig 1 C,D). In the rigid flatfoot the arch does not reconstitute when the child is non-weight bearing nor when the child does a heel rise. These cases should be referred on for an orthopaedic consult to rule out a tarsal coalition or vertical talus.
The flexible flatfoot can be further divided into two subgroups: The symptomatic (symptoms) flexible flatfoot and ssymptomatic (no symptoms) flexible flatfoot.
The symptomatic flexible flatfoot will have symptoms as alluded to earlier, which does not necessarily have to be painful. These symptoms can include an avoidance of activities, frequent request to be carried, an awkward gait in comparison to peers, or an inability to keep up with peers. It is important to keep in mind that children with flexible flat feet may not be able to convey symptoms verbally to parents or practitioners. Children that have symptomatic flexible flatfoot certainly benefit from conservative treatment with orthotics and proper footwear.
The asymptomatic flexible flatfoot, or symptom-free flexible flatfoot, accounts for the majority of children. These type of feet typically require no treatment3. In cases where the child’s foot mechanics fall outside the range of what they will grow out of, then regular monitoring is advised. In cases where there is a family history of foot problems conservative treatment with orthotics and proper footwear may be warranted.
Other factors that can impact the arch development of children include obesity, family history, and ankle equinus (decreased upward bending at the ankle).
For more information about this and other paediatric foot issues, contact the team at Applied Biomechanics to find out how we can help.
1Valmassy RL. Biomechanical evaluation of the child. Clin Podiatry. 1984; 1(3):563-79.
2Butterworth ML. A Systematic Approach to Pediatric Flatfoot: what to do and When to Do It. Podiatry Today December 2009
3Scherer PR. Treatment of Pediatric Flexible Flatfoot with Functional Orthoses. Podiatry Management CME September 2008